Introduction
Mubende Regional Referral Hospital (RRH) is a 229-bed hospital located in the Western Central Region of Uganda and serves people in the districts of Mubende, Mityana, Kassanda, Kiboga, Kyankwanzi, and parts of Kyegegwa, Kibaale, Sembabule, Kakumiro, and Gomba. The hospital was elevated to a Referral Status in FY2009/2010, serving a district population of 611,900 (UBOS Projection of 2022).
- Annual Outpatient Department (OPD) attendance 2021 average: 82,516
- Annual Antenal Care (ANC) attendance average: 8,083
- Annual deliveries average: 5,710
- Annual pediatric admissions average: 1,716

About the Ebola Situation
On the 20th of September, Uganda declared an Ebola disease outbreak caused by the Sudan ebolavirus species after confirmation of a case in Mubende District. Case fatality rates of the Sudan strain have varied from 41% to 100% in past outbreaks. Early initiation of supportive treatment has been shown to significantly reduce deaths from Ebola. The confirmed case was from a sample taken from a 24-year-old male. This investigation was triggered by six suspicious deaths that occurred in the district of Mubende in the same month. During this outbreak, there were 164 cases (142 confirmed and 22 probable), 55 confirmed deaths, and 87 recovered patients in total.
The World Health Organization (WHO) and partners supported Uganda health authorities from the onset of the outbreak, deploying experts; providing training in contact tracing, testing, and patient care; building isolation and treatment centers; and providing laboratory testing kits. In addition, the president announced directives to support the control of Ebola transmission, including prohibition of movements into and out of the Mubende and Kasanda Districts for 21 days starting on the 16th of October 2022.
Ebola Summary Report
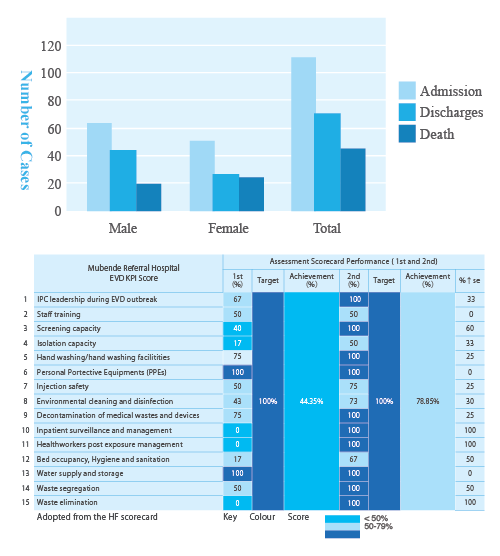

During this Ebola outbreak at Mubende RRH, six healthcare workers tested positive for Ebola. The outbreak spread to nine districts in Uganda (Mubende, Kyegegwa, Kassanda, Kagadi, Bunyangabu, Kampala, Wakiso, Masaka City, and Jinja). Rapid response teams were deployed to support outbreak response activities, including the investigation of unexplained deaths and contact tracing. The CDC provided support for surveillance, epidemiology, laboratory, communication, and ecological investigations. On the 11th of January 2023, Uganda declared the end of the outbreak.
About Infection Prevention and Control (IPC) in Mubende Regional Referral Hospital
- In Mubende RRH, the IPC committee has been in existence since 2010, but hand hygiene practice was not being practiced as per standard following the five moments until 2016.
- There were no guidelines, posters, or trainings specifically targeting hand hygiene in place.
- The main emphasis was placed on the availability of PPEs, the decontamination process, and waste management.
- Meetings and supervisions were irregular but still focused on the above elements and not hand hygiene.
- In 2016, hand hygiene practices began with the support of Infectious Diseases Institute (IDI) and SARAYA.
- External and internal training was conducted. SARAYA supplied and installed alcohol hand disinfectant dispensers with alcohol hand disinfectant in all units.
- The IDI and Uganda National Medical Stores (NMS) provided materials for manufacturing alcohol hand disinfectant in the hospital.
- Uganda Continuing Medical Education (CME) and meetings with refreshments and facilitation were initially supported by the IDI up to 2019.
- Sustainability was ensured by continuous mentorships and support supervision on hand hygiene compliance.
- During the COVID-19 outbreak, hand hygiene was generally at its peak by healthcare workers, patients, and their attendants.
- During the COVID-19 outbreak, hand hygiene was generally at its peak by healthcare workers, patients, and their attendants.
- Data collection on hand hygiene compliance was not conducted during the COVID-19 outbreak.
- During the Ebola disease outbreak, there was no transmission to patients via healthcare workers due to a reduced number of patients because of lockdown, adequate supply of PPE from partners, and high hand hygiene compliance.
The Goal
- Protect the patient against harmful germs carried on our hands.
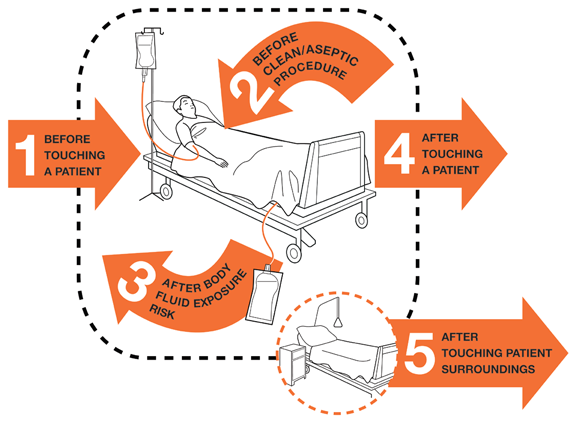
- Protect ourselves and the healthcare environment from harmful germs by practicing the five moments of hand hygiene.
IPC Baseline Assessment
- Knowledge gap
- Few handwashing facilities with soap
- No alcohol hand disinfection practice
- Gloving only with no hand hygiene action
- All units had pathogens on their surfaces, including theatre and neonatal units
- IPC posters on hand hygiene were totally lacking
Strategies to reduce Healthcare-Associated Infections (HAIs) and antimicrobial resistance
- Training of HOD (head of department) and in-charges by IDI
- Formation of a vibrant IPC team that received formal appointments
- Development of action plans concerning training, CME, and supervision
- Institutional process of alcohol hand disinfectant
- Display of standard operating procedure for hand hygiene
- Monthly hand hygiene monitoring using the WHO assessment tool
- Awarding of best-performing units
- Performance and dissemination of monthly analysis of the hand hygiene compliance rate for the hospital
- Quarterly monitoring of hand hygiene alcohol disinfectant consumption
- Daily sensitization of patients, clients, and attendants to hand hygiene
- Continuous orientation of all staff and students
- Monthly meetings to review performance and formulate action plans
- Radio talk shows
- Provision of handwashing facilities by UNICEF during the COVID-19 outbreak
Hand Hygiene Compliance
Pictures of IPCC training.

Methods for Monitoring
The following methods were used by the hospital IPC committee on hand hygiene:
- Observational
- Investigative – swabbing
- Cross-sectional survey – baseline data
- Use of a checklist
Compliance
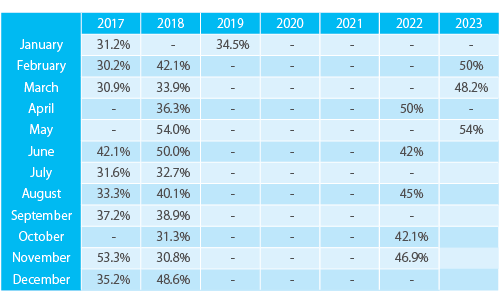
Baseline on 16th of December 2016: 21.6%
January 2019 : 34.5%
November 2021 : 40%
April 2022 : 50%
Patterns of Transmission of Reduce Healthcare-Associated Infections (HAIs) Continued
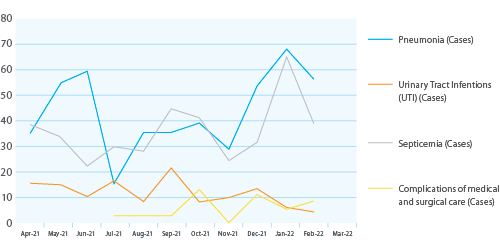
- In July 2021, there was a decrease in pneumonia cases. This could be associated with increased hand hygiene during the COVID-19 outbreak.
- In November/December 2021, there was a rise in all cases. This could be attributed to the laxity in the observance of hand hygiene. There was a decrease in septicemia and pneumonia cases from January 2022 to April 2022. This could be due to the increased number of training sessions on hand hygiene for both the students and staff for the period.
- September-November 2022, due to the Ebola outbreak, the number of patients dropped dramatically due to the lockdown, and IPC committee members joined the Ebola Treatment Unit.
Challenges
Despite hospital hand hygiene compliance being above the WHO target, the following factors are affecting hospital hand hygiene compliance.
- Individual factors (too busy/workload, skin irritation, glove use, the “don’t think about it” attitude)
- Inadequate functional handwashing facilities and dispensers
- Irregular supervision in some units
- Stockouts of alcohol hand disinfectants
- Transfer of trained staff to other hospitals
Recommendations
- Continuous mentorships of all students and staff on hand hygiene
- Constant supply of alcohol hand disinfectant manufacturing materials by NMS and the Ministry of Health
- All units should have functional taps and a constant water supply
- Continuous monthly assessment and meetings to measure hand hygiene compliance
- Continuous verbal reminders to health workers who are laggards
Conclusions
- Hand hygiene is crucial in the prevention of HAIs. The use of gloves does not replace the need to clean your hands.
- On-site mentorships/CME of all students and staff about hand hygiene have improved hand hygiene compliance from 21.6% in 2016 to 54% as of May 2023.
-
Publication Date:December 12, 2023
-
Category:Hand Hygiene
HosCom International 2023 Vol. 2
