Introduction
Hand hygiene is widely regarded as a fundamental aspect of clinical practice, serving as an indispensable measure for the prevention of healthcare-associated infections (HAIs) and the spread of antimicrobial resistance (AMR). In 2009, the World Health Organization (WHO) issued guidelines on hand hygiene, emphasizing the need for a comprehensive approach to instituting behavioral change in this area1. The WHO Multimodal Hand Hygiene Improvement Strategy (MMIS) is an evidence-based approach designed to promote a hand hygiene behavioral change among healthcare workers. The MMIS comprises five key elements: system change, education and training, monitoring and feedback reminders in the workplace, and institutional climate change.
It is important to note that individual interventions, such as the installation of alcohol-based hand rub (ABHR) dispensers in wards or monitoring hand hygiene compliance among healthcare workers, are insufficient to promote hand hygiene effectively at the facility level. Thus, a more systematic approach is required to implement proper hand hygiene practices using the MMIS strategy, essential to which are education and training. As stipulated by the WHO guidelines, all healthcare workers require comprehensive education and training on hand hygiene. As such, by employing a user-centered, standardized approach to disseminate clear messages, such training and education can foster behavioral and cultural changes, ensuring that hand hygiene competency is deeply ingrained in and maintained among all healthcare workers. Furthermore, the WHO published a research agenda concerning hand hygiene in healthcare in 2023, which included 21 high-priority research statements following extensive expert consultations and consensus agreement processes2. One of these statements aimed "to evaluate the impact of different hand hygiene training and educational strategies on the knowledge and skills of health and care workers across all levels of the healthcare system.” Therefore, the pursuit of an effective training approach remains a key focus within the "education and training” domain.
What is the TTT in hand hygiene? Course structure and strategy
The Train-the-Trainers (TTT) course is a standardized approach to hand hygiene training for infection prevention and control (IPC) professionals3, originally launched by the University Hospitals of Geneva (HUG) as a WHO Collaborating Centre (WCC). This three-day practical training program is based on the WHO MMIS (Figure 1).
The course consists of didactic lectures, hands-on sessions with video reviews of clinical scenarios, role-playing of clinical scenarios, and the mutual exchange of successful experiences and challenges faced by the participants in their clinical settings, with the aim of enhancing interactions and discussions between participants and lecturers. The materials developed for the course include videos and case scenarios for role-playing, and the original course is facilitated by IPC practitioners trained and validated in hand hygiene by IPC/WCC faculty members and local IPC focal points in their respective countries. Simulation-based sessions focus on the direct observation of hand hygiene compliance monitoring according to the WHO's “My 5 Moments,” using video reviews of clinical scenarios and role-playing.
The key aspects of the course include the impact and burden of HAI and AMR; the advantages and disadvantages of direct observation, automated electronic monitoring, or a combination of both; feedback from the course participants on the direct observation of the WHO’s "My 5 Moments”; barriers to hand hygiene practices, such as gloves, nails, jewelry, and skin problems; and an education and validation plan for hand hygiene observers, with inter- and intra-rater reliability testing (optional). In addition, improvements in participants' knowledge of hand hygiene throughout the course were assessed using a pre- and post- course evaluation.
The course is designed to enhance participants’ knowledge, to share experiences, and to expand networks, and IPC professionals who have participated in the course can use this reference training method to disseminate knowledge further to other healthcare workers (that is, the concept of "trainees becoming trainers"). All course materials are made available for modification and adaptation by course participants to encourage the organization of subsequent TTT courses, and they are currently available in English and Spanish. In addition, the course content is translated into local languages, and simultaneous interpretation is provided for non-native Englishor Spanish-speaking countries, where necessary, as the TTT course, first launched in 2016, has been conducted across four continents (Figure 2). Course lecturers and local organizers are present at all times throughout the course to answer any questions related to the interpretation of information.
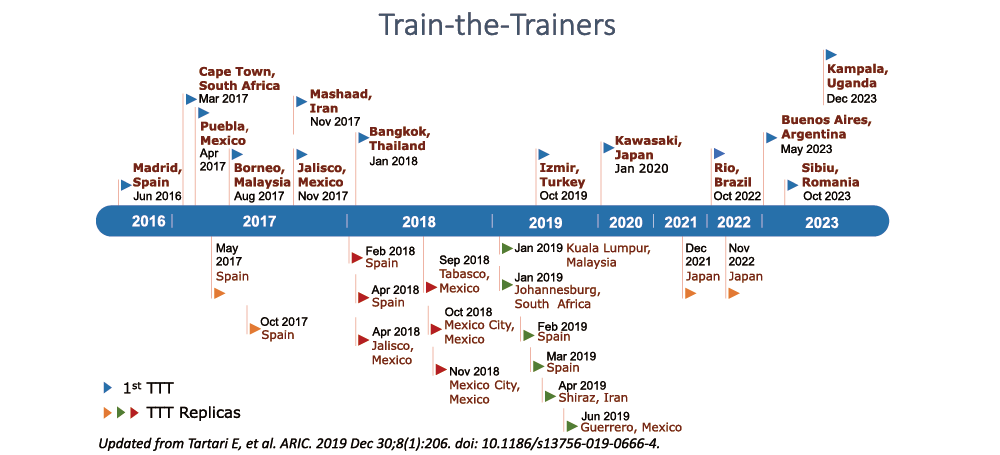
Timeline chart showing the evolution of the TTT course between June 2016 and December 2023. *Replicas are organized by former TTT program participants and local IPC organizers. Note: The term TTT program depicts the overall process, including the original first courses and replicas.
General findings at the global level
Tartari et al. conducted a study examining the effects of the TTT course on hand hygiene knowledge in six countries: Iran, Malaysia, Mexico, South Africa, Spain, and Thailand3. The target audience was professionals involved in IPC at healthcare facilities, and the evaluation utilized a pre- and post-training questionnaire to assess knowledge related to microbial transmission, hand hygiene principles, and the WHO methodology for hand hygiene monitoring. The study found that 305 IPC professionals completed the TTT course across over 20 countries, as well as observed a significant improvement in hand hygiene knowledge following TTT course completion in all participating countries. The positive aspects of training include a unique learning environment, experience sharing, hands-on practice, and networking among IPC professionals. The study revealed further that the knowledge improvements were sustained in follow-up evaluations conducted five months to two years after the initial course. As such, this study's global impact is considerable, demonstrating the effectiveness of the TTT model in significantly improving hand hygiene knowledge among healthcare professionals, which is crucial for driving progress in IPC. Further, the success of the TTT model in diverse countries indicates its adaptability and relevance across different healthcare systems and cultural contexts.
The TTT model, which equips individuals to instruct others, has evidenced considerable improvements in hand hygiene compliance and comprehension across diverse healthcare settings, and the approach is particularly beneficial in resource-constrained environments, providing a cost-effective and scalable solution to bolster infection control practices. This study accentuates the crucial function of standardized, all-encompassing training in cultivating a culture of safety and cleanliness in healthcare settings on a global scale.
Local adaptation, adoption, and cascading effect: Mexico
The hand hygiene TTT training approach was first offered in Mexico by the HUG team on two occasions, in April and November 2017, training 84 healthcare professionals as hand hygiene leaders in Mexico. The course was delivered mostly in Spanish by Spanish-speaking lecturers from the HUG team using translated materials. The commitment established by the leaders who received training implied the responsibility of continually promoting the training and adapting it to the different contexts and needs in other regions and institutions of the Mexican health system. Thus, a cascading effect was evidenced: in total, 278 health professionals were trained over five training workshops conducted in the states of Jalisco, Tabasco, Mexico City, and Guerrero between 2018 and 20193.
The training of health professionals in hand hygiene is critical for the consolidation of IPC teams in health facilities, involving the 8 basic components of IPC, which are taken as starting points. In the case of Mexico, 15 IPC initiatives were identified, including the necessity for regulatory frameworks or manuals and guidelines that encourage training in different aspects, including hand hygiene4. Bedside implementation, however, needs a continuation of the training cascade. Next steps should include a consistent and standardized competency validation process for hand hygiene trainers and observers to ensure the correct application of the MMIS.
Local adaptation, adoption, and scaling up: Japan
The TTT course was first conducted in Japan by the HUG team in January 2020, for which the original TTT materials were translated into Japanese where appropriate, and several Japanese physicians helped the HUG lecturers deliver the course as interpreters. Satisfaction among about 80 participants was overall high, but a few challenges were identified based on a course satisfaction survey. The first was related to the language barrier: despite the translated materials and live translation, most Japanese participants spent much energy interpreting comments by lecturers word-for-word. In addition, each lecture took longer because of multiple interruptions in the live translation, and time management in the course delivery was difficult. The second challenge was related to the different contexts of healthcare across countries. For example, some simulation videos were created in the Swiss healthcare setting, causing some participants difficulty in applying the videos to their own healthcare contexts.
Therefore, modifications were made in 2021 and 2022, where participants who wanted to become "trainers" were recruited from among the first TTT participants ("trainees") to formulate a team: "TTT-Japan." Regular meetings were held monthly, and the team created an agenda to improve the TTTs and update their progress. They modified the TTT program slightly in consultation with the HUG team so the content would be of even greater interest to Japanese participants while maintaining the original teaching points intended to be delivered. Other activities included the standardization of Japanese terms to be used for the WHO MMIS and the creation of simulation videos elaborated in a Japanese healthcare setting. Due to the COVID-19 pandemic, the team transitioned its course delivery to hybrid (on-site and online) in 2021 and 2022, respectively, leading not only to consistent knowledge improvements between the pre- and the post-course period among TTT participants, but also to trainers' further contributions to institutional climate change in their own facilities. (5) TTT-Japan provided a space in which trainers could work on hand hygiene promotion as a team and learn from each other; as a result, they gained more confidence in hand hygiene promotion activities at their own facilities, including leadership engagement.
Local alcohol-based hand production, adaptation, and adoption: Uganda
Most recently, in December 2023, the TTT course was conducted in Uganda, offered for the first time in a low-income African country, as historically, the Japanese International Cooperation Agency (JICA) contributed to patient safety in Uganda. Hand hygiene promotion was selected as the first Global Patient Safety Challenge by the WHO in 2005, and it was highlighted as an important patient safety agenda in Uganda. The TTT was officially organized by the Ministry of Health (MOH) in Uganda in December 2023 with the support of the JICA, in which more than 40 IPC focal points or IPC professionals participated across 18 regional referral hospitals, as did major stakeholders, including several collaborators from the MOH, such as high-level colleagues. The demand for IPC training and education was excessive, and participants and lecturers exchanged approaches to improve hand hygiene in resource-constrained settings. Many participants also worked on quality improvements and patient safety at their facilities, suggesting that the TTT course's impact would be reinforced by the close linkage with other key horizontal activities, such as patient safety.
Importantly, the MMIS cannot be implemented without a pre-requisite system change, i.e., the universal availability of the ABHR solution at the point of care, facilitated in Uganda by the long-term planned local production of ABHR from sugar cane byproducts in Jinja, in the middle of the country. The successful partnership between the Kakira sugar factory and Saraya Manufacturing (U) Ltd., for more than 10 years has made it possible for the MMIS to be implemented in several hospitals in Uganda and, in particular (but not only) in hospitals involved in the MIKONO study in four locations of the East part of Uganda: Kumi, Mbale, Tororo, and Busia.
Conclusion and Perspectives
Hand hygiene promotion is a never-ending process, and as such, the TTT will continue to be delivered by the HUG team, as well as by TTT-trained local teams across the globe, creating a cascading, or even snowballing effect. "Adapt to adopt" is key to this success, so the TTT course content and its mode of delivery will continue to be adapted, maintaining the standard concept of the WHO MMIS, built upon the multimodal strategy developed at HUG in the 1990s. In addition, the TTT format can be utilized in other IPC areas, such as environmental cleaning. Now that the TTT network has been expanding globally, its potential to impact IPC in healthcare is significant. Thus, we hope more and more IPC professionals and frontline healthcare workers will join, adapt, deliver, and spread TTT knowledge, thus contributing to patient safety altogether as a global team effort.
-
Publication Date:October 04, 2024
-
Category:Hand Hygiene
HosCom International 2024 Vol. 2
